

INTRODUCTION
Among adolescents, depression and suicide are principal causes of illness and death, respectively [1]. Adolescent depression is associated with poor school attendance. It inhibits normal growth and development [2] and increases risk of suicide [3]. Furthermore, adolescent depression can lead to the occurrence of chronic and severe depression and other psychiatric comorbidities in early-to-middle adulthood, affecting personal health status and public health expenditure [4,5]. One-third of individuals with depression initially experience its symptoms during adolescence and young adulthood. Hence, appropriate interventions are required [6].
Previous systematic reviews on adolescent depression have predominantly included studies conducting face-toface interventions with adolescent individuals, their families, and groups [7,8]. Providing face-to-face psychosocial treatments is effective in improving symptoms of subjects experiencing depression [8]. Representative interventions of psychosocial therapy include interpersonal psychotherapy and cognitive behavioral therapy (CBT) [8]. In addition, psychoeducational interventions providing knowledge and self-management strategies for adolescent depression are effective in reducing depression and improving mental health outcomes [7].
Despite the effectiveness of face-to-face services, the use of face-to-face mental health services by adolescents with depression is less than 40% [9]. Prominent barriers to accessing face-to-face mental health services for adolescents include perceived stigma and negative attitudes and beliefs toward mental health services [10]. On the other hand, adolescents perceive online interventions positively and believe that online interventions can alleviate stigma and increase access to therapies [11]. Online platforms are alternatives to reduce barriers to availing face-to-face services for mental health. High accessibility of online platforms to adolescents is important because traditional face-to-face services for mental health have low accessibility and engagement [12]. Furthermore, due to the COVID-19 pandemic that is continuing, mental health services are provided online as a convenient and safe way of reducing face-to-face contact [13].
One systematic review has reported that mental health interventions using mobile applications and technologies have positive effects on engagement and emotional self-awareness among children and adolescents [14]. Web-based and mobile application interventions for suicide prevention have shown good acceptability and satisfaction among adolescents [12]. Although previous meta-analysis studies have revealed that online interventions are effective in improving depression [15,16], these reviews were restricted to web-based interventions [15] or included only adolescents ≤18 years [16]. As it becomes convenient to use smartphones to monitor depressive symptoms, collect objective and subjective data, and send reminders, mobile interventions for adolescents with depression are rapidly increasing [17]. With delays in transition to adult roles and responsibilities including completion of education, marriage, and parenthood, extending the age of adolescence to the 20s is more appropriate from the point of view of the life phase in the current society [18]. To address this existing gap, we systematically reviewed interventions using website and mobile application for adolescents and young adults with depression. Furthermore, we evaluated the effectiveness of these interventions using meta-analysis and the effectiveness by intervention type, delivery method, and assessment time point through subgroup meta-analyses.
METHODS
2. Eligibility Criteria
The following studies were included: (a) studies on adolescents or young adults, 13 to 25 years; (b) studies on adolescents or young adults diagnosed with depression or have symptoms of depression; (c) studies on interventions to improve mental health status or treat mental health problems; (d) studies employing websites or mobile application-based interventions; (e) studies presenting a comparison group; (f) studies reporting an outcome evaluating depressive symptoms; (g) randomized controlled trials (RCTs); and (h) published English articles from January 2010 to April 2021. Studies were excluded if they included individuals aged ≥26 years or ≤12 years or did not report information on participants’ age range. Intervention studies without randomization, reviews, study protocols, editorials, national and international reports, conference proceedings, and grey literature were also excluded.
3. Information Sources and Search Strategy
Databases searched (on April 14, 2021) included Pub-Med, Cochrane Library CENTRAL, and EMBASE. A medical librarian assisted with the development of a search strategy. Search strategies included the following keywords: “adolescent”, “young adult”, “intervention”, “therapy”, “program”, “mobile application”, “online”, “website”, “depression”, “randomized controlled trial”. The search period was from January 2010 to April 2021. Only articles written in English were included. Our search strategies are presented in Supplementary File S1.
4. Selection Process
Duplicates articles were removed. Two researchers independently reviewed the title and abstract of the article to assess their eligibility. After reviewing eligible full-text articles and discussing their inclusion, final articles were selected. Disagreements on study selection were resolved by discussion until reviewers reached a consensus. If needed, researchers discussed with a third reviewer.
5. Data Extraction
Before data extraction, two reviewers developed a data extraction form tailored to the review question through discussions. Items such as author, country, publication year, target population, participants’ and intervention characteristics, study design, comparison condition, measures of depressive symptoms, assessment time points, results, and data related to risk-of-bias were extracted from each study. Data extraction was performed by two independent researchers. Disagreements were discussed with a third reviewer to reach a consensus. All data were extracted from every source if there were multiple publications of one study.
6. Risk-of-Bias Assessment
Two independent researchers evaluated each study using the Cochrane risk-of-bias tool for randomized trials, version 2[21]. After evaluation, two researchers discussed disagreements and reached consensus. Each researcher evaluated each domain of bias and then selected one of five response options: “yes”, “probably yes”, “probably no”, “no”, and “no information”. The risk of bias for each domain was classified as “low”, “having some concerns”, or “high”, depending on responses to signaling questions. By integrating evaluation results for each domain, the overall risk of bias was judged as “low”, “having some concerns”, or “high” for each study. Egger’s regression test [22] was used to estimate publication bias.
7. Effect Measures and Synthesis Methods
Summary statistics extracted from examined studies included post mean values, standard deviations (SDs), and sample sizes of intervention and comparison groups. We calculated SDs from standard errors or 95% confidence intervals (95% CIs) of means when SDs were unreported in studies [23]. When separate summary statistics for two subgroups in a group were reported, we combined them into sample size, mean, and SD for a single group using formulas [23]. If a study used two or more psychometric scales to measure depressive symptoms, we selected summary statistics of a primary scale for meta-analysis. When a study presented several intervention conditions, we selected the most appropriate intervention to reduce depression and extracted summary statistics of an intervention group.
Through meta-analysis, we evaluated the overall effect of interventions using a website and mobile application on depressive symptoms at posttest. We then conducted a subgroup meta-analysis by combining studies according to distinguishing characteristics of included interventions such as intervention type (internet-based CBT (ICBT) and non-ICBT) and intervention delivery method (website and mobile application). Furthermore, to evaluate long-term effects, we conducted a separate meta-analysis for assessment time points such as 3-, 6-, and 12-month follow-up time points. For meta-analyses, we used Comprehensive Meta-Analysis Version 3 software (Biostat, Englewood, NJ, USA). Effects are presented using the effect size of Cohen’s d value and 95% CI. We used a random-effects model with DerSimonian and Laird method [24] because of heterogeneity across included studies. We used I2 statistic to measure statistical heterogeneity.
RESULTS
1. Study Selection
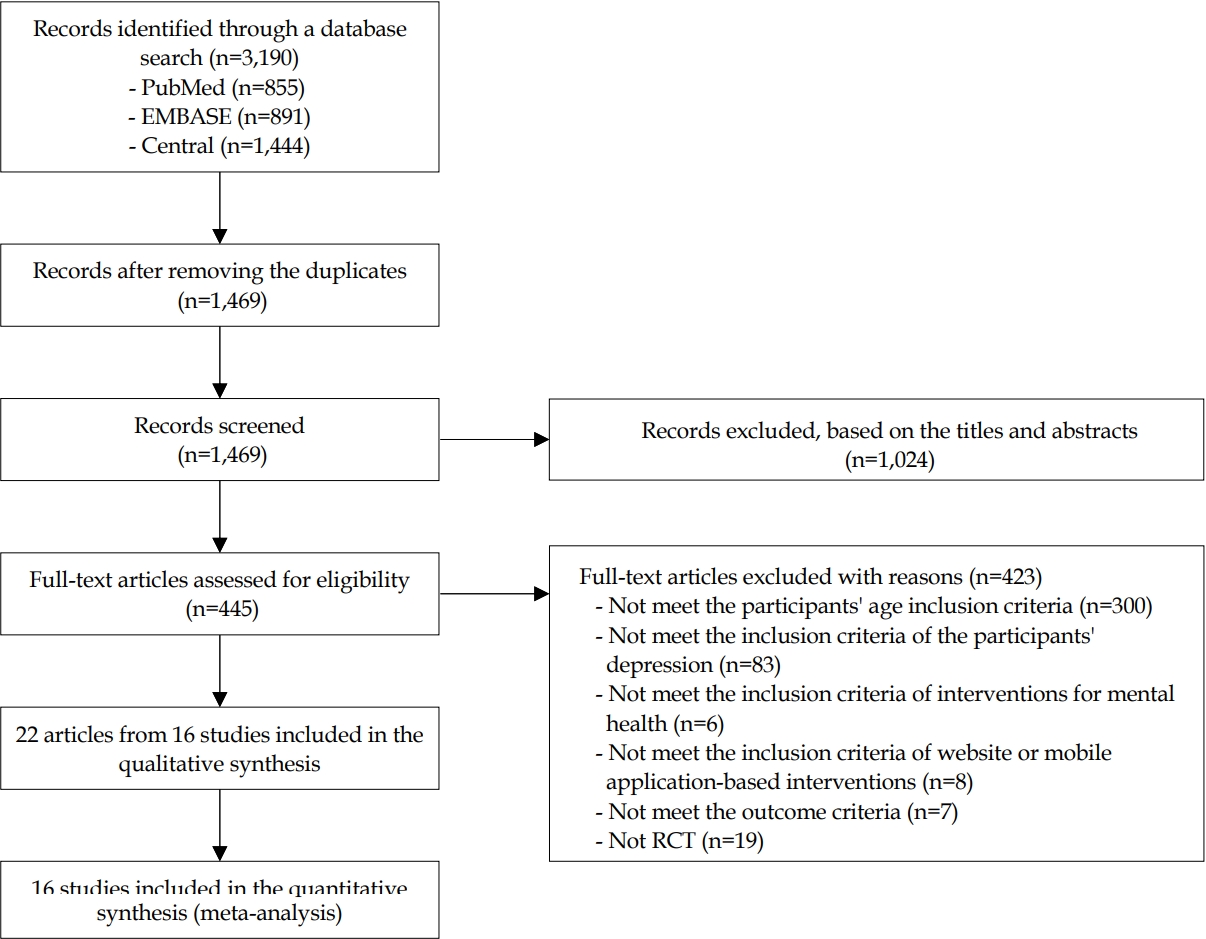
After removing duplicates, 1469 articles remained. By screening titles and abstracts, 1024 articles were excluded. After assessing 445 full-text articles, 423 were excluded. Finally, 22 articles from 16 studies were included in this review (Figure 1).
2. Study Characteristics
Characteristics of each study are presented in Table 1.
The sample size varied from 21 to 369, with participants’ age ranging from 13 years to 25 years. For depression severity, it was mild to moderate depression in five studies [A1-A5], mild to severe depression in five [A6-A12], and moderate depression in two [A13-A16]. Moreover, one study involved participants at risk of depressive disorder through interview with primary care physicians [A17-A19]. Two studies [A20,A21] targeted participants diagnosed with major depressive disorder and one study [A22] targeted those with suicidal ideation.
Regarding intervention contents, among 11 studies using Internet-based CBT (ICBT), five [A1,A3-A5,A22] used ICBT only and six [A2, A6, A7, A12-A19] incorporated ICBT with other intervention strategies. Among these six studies, three [A2,A14-A19] used CATCH-IT (Competent Adulthood Transition with Cognitive Behavioral Humanistic and Interpersonal Training) program which incorporated ICBT, behavioral activation, interpersonal psychotherapy, and intervention based on a community resiliency concept model. Furthermore, two studies [A6,A7,A12] used ICBT blended with chat-based psychological support and one study [A13] used motivational interviewing. Besides ICBT, other interventions were adopted in previous studies. The intervention delivery method was website-based in 14 studies and mobile application-based in two [A9-A11].
Eight studies provided reminders to increase participants’ treatment adherence. Reminder delivery cycles included before each session [A3,A5,A12], daily [A9], weekly [A8], monthly [A2], random intervals [A10,A11], and when participants’ assessments were incomplete [A13]. These reminders were provided through emails [A8,A13], phone calls [A2], text messages [A3,A9], messages through social media [A2], or auditory signals from a mobile phone [A10].
Twelve studies reported participants’ treatment adherence. Among seven studies [A1,A2,A4,A6,A7,A14-A16,A21,A22] assessing treatment adherence as participant proportion in the intervention group who completed whole sessions, four studies [A1,A4,A6,A7,A21] reported that ≥50% completed whole sessions. However, other studies reported approximately completion rates of 30.8% [A22], 10.1% [A2], and < 10% [A14-A16]. On the other hand, three studies [A12,A13,A17-A19] assessed treatment adherence as the proportion of participants who completed 50% of interventions. Additionally, two studies [A9-A11] assessed the proportion of participants who met a set of minimum requirements.
For the assessment of depressive symptoms, thirteen measurements were used. The most frequently used measurement was the Center for Epidemiologic Studies Depression Scale (n=6). Patient Health Questionnaire-9 and Beck Depression Inventory-II were each employed in four studies, respectively. Children’s Depression Rating Scale-Revised was used in three studies and Depression Anxiety Stress Scale-21 Items was used in two studies.
3. Estimated Risk of Bias
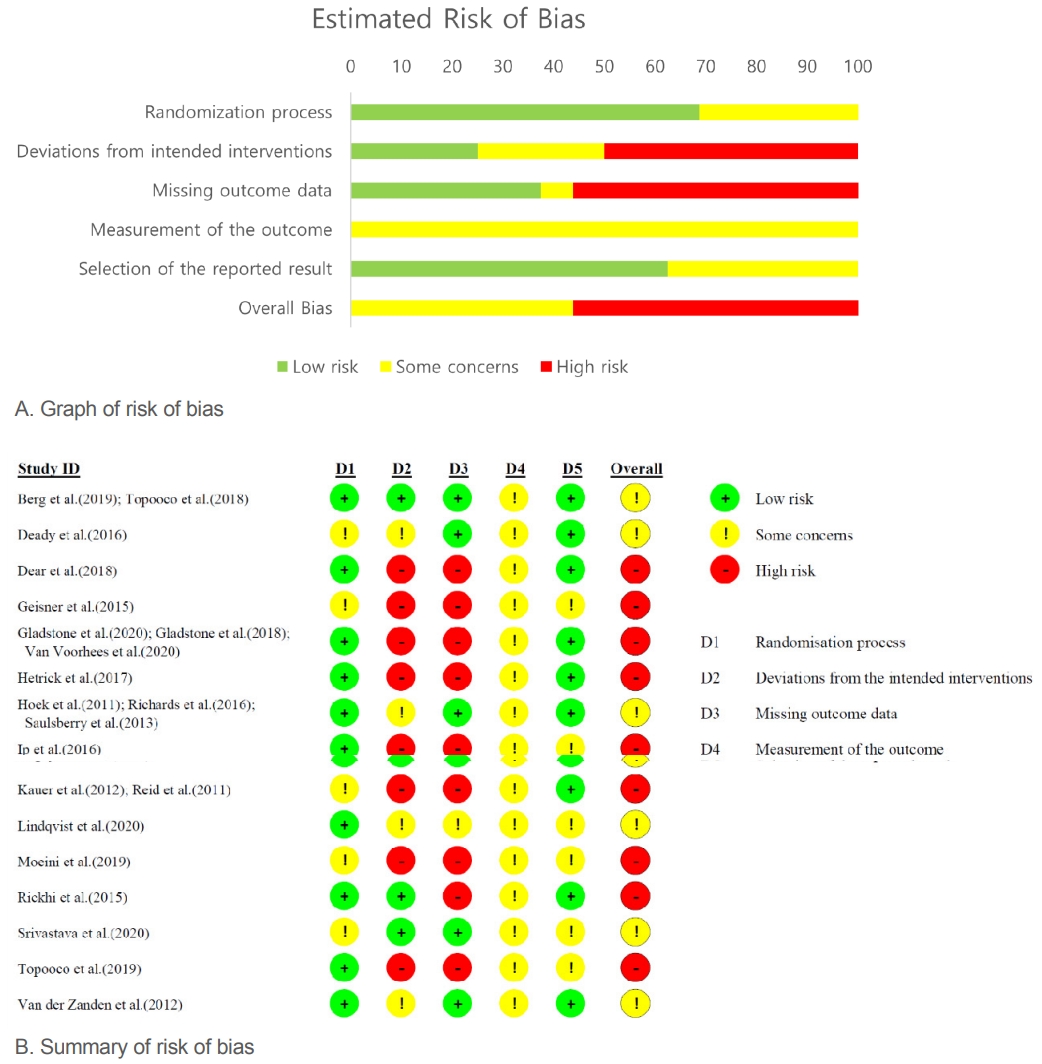
Figure 2 shows the estimated risk-of-bias. Overall, 9 studies [
A1-A3,A8,A10-A12,A14-16,A21,A22] had a high risk of bias and 7 studies [A4-A7,A9,A13,A17-A20] had some concerns. A high risk of bias because of deviations from the appointed interventions was identified because blinding was not performed when participants were allocated to the intervention and deviations from targeted intervention were disproportionate between intervention and comparison groups [A1-A3,A8,A10-A12,A14-16,A22]. In addition, missing data on the outcome variable and different reasons for attrition rates and dropout between intervention and comparison groups were reasons for the risk of bias [A1-A3,A8,A10-A12,A14-16,A21,A22]. No publication bias was shown in Egger’s regression test results at the posttest or 3-, 6-, 12-month follow-ups (p =.274, .184, .787, and .715, respectively).
4. Estimated Results of Meta-Analysis
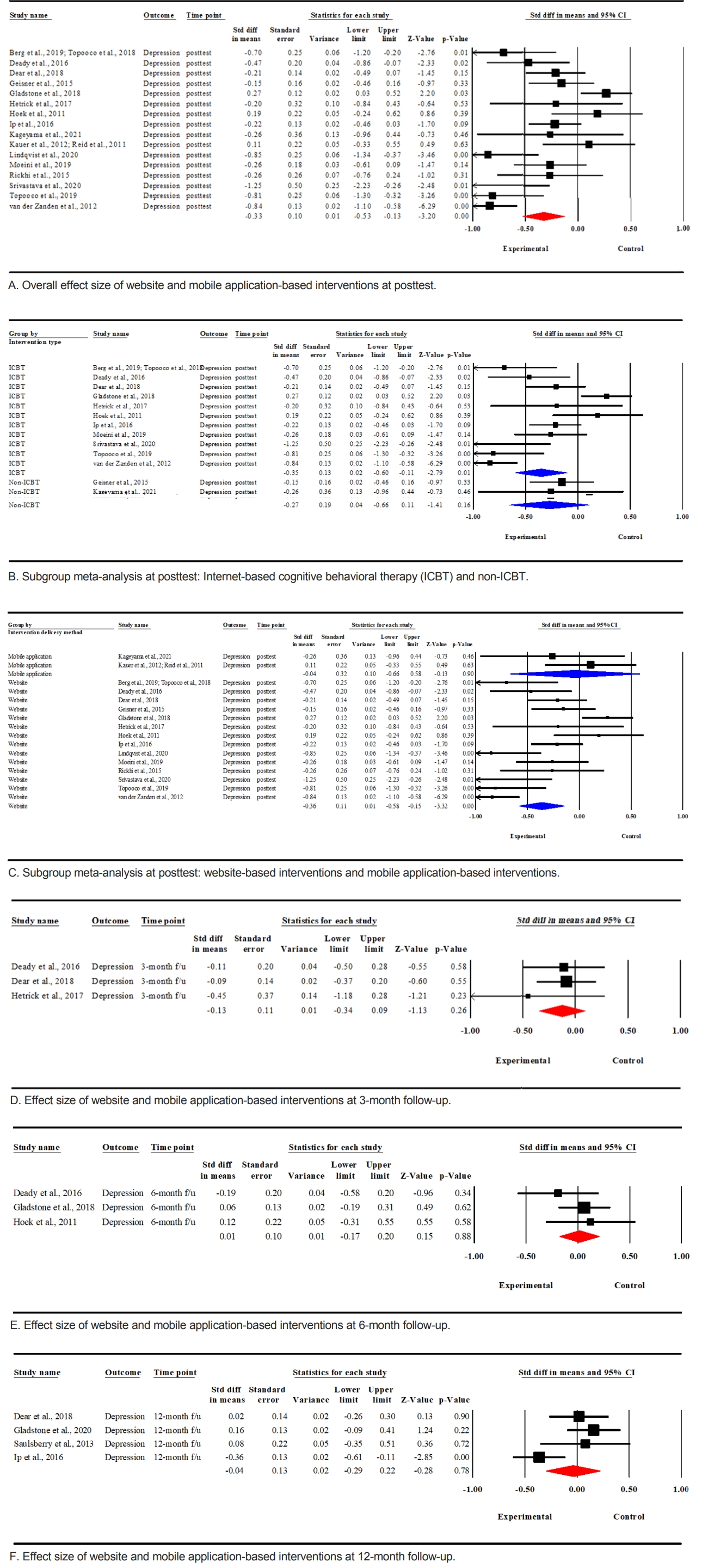
Figure 3 presents effect size of interventions on depression using forest plots. Random-effects meta-analysis combined 16 studies employing website and mobile application-based interventions. It showed that intervention had significant beneficial effects on depressive symptoms (d=-0.33, 95% CI: -0.53 to -0.13) at posttest. The meta-analysis had a considerable heterogeneity (I2=76.4%).
All included studies were grouped by intervention type(ICBT and non-ICBT) before conducting subgroup meta-analyses. After combining 11 studies employing ICBT, significant differences in depressive symptoms for ICBT over the control were shown (d=-0.35, 95% CI: -0.60 to -0.11, I2=81.6%). A subgroup analysis combining five studies not employing ICBT showed no significant difference in depressive symptoms between groups (d=-0.27, 95% CI: -0.66 to 0.11, I2=55.1%).
Additionally, included studies were classified by intervention delivery method (i.e., websites and mobile application). A subgroup analysis combining 14 studies revealed that website-based interventions resulted in significant differences in depressive symptoms between intervention and control groups (d=-0.36, 95% CI: -0.58 to -0.15, I2=78.5%). Whereas a subgroup analysis combining two studies employing mobile application-based interventions showed no significant difference in depressive symptoms between intervention and control groups (d=-0.04, 95% CI: -0.66 to 0.58, I2=0%).
We pooled studies with 3-, 6-, and 12-month follow-up time points to assess long-term effects of interventions using website and mobile application. A meta-analysis combining three studies [A1,A13,A22] with 3-month follow-up showed no significant effect of intervention on depressive symptoms (d=-0.13, 95% CI: -0.34 to 0.09), with minimal variation (I2=0%). Additionally, there was no significant effect on depressive symptoms in a meta-analysis synthesizing three studies [A13,A15,A17] with a 6-month follow-up (d=0.01, 95% CI: -0.17 to 0.20, I2=0%) or four studies [A1,A2,A14,A19] with a 12-month follow-up (d=-0.04, 95% CI: -0.29 to 0.22, I2=67.5%).
DISCUSSION
This study conducted a systematic review and meta-analysis of online-based interventions, including website and mobile application, for adolescents and young adults with depression. ICBT was the most frequently used intervention strategy among various intervention strategies we identified. It was used in 11 of 16 studies reviewed. Furthermore, there were more studies employing incorporated ICBT with other intervention strategies than using ICBT only.
Our meta-analysis showed that website and mobile application-based interventions significantly reduced depressive symptoms (d=-0.33). Our sub-group meta-analysis combining studies that employed ICBT showed a significant effect of intervention on depression (d=-0.35), while non-ICBT showed no significant effect on depression. This result concurred with a result of previous meta-analysis showing an effect of ICBT for adults with insomnia on comorbid depressive symptoms (d=-0.36) [25]. CBT is known as the most researched, systematic, and best standard psychological treatment [26]. The use of ICBT is also supported by a previous study reporting that ICBT has the largest effect size among technology-delivered interventions for depression and anxiety [16].
However, the effect size of ICBT in this review (d=-0.35) was lower than the effect size of a previous review synthesizing studies that conducted CBT using face-to-face and online formats for children and adolescents with depression (d=-0.41) [27]. Although the evidence supports the use of ICBT, given that the effect size was small, increased efforts such as therapeutic supports using video calling or texting are necessary to effectively implement CBT using website and mobile application formats [28].
Our review found that most studies employed website-based interventions except for two studies that employed interventions delivered via mobile applications. Consistent with our results, a previous systematic review has reported that although mobile application delivery method might be preferred by adolescents and young adults over a web-based method, evidence of their effectiveness is insufficient [29]. Further RCTs of interventions using mobile application are needed to evaluate the effectiveness through quantitative synthesis.
Our results showed that effects of online interventions on depressive symptoms at posttest were significant, but not in long-term follow-up assessments. Subgroup meta-analyses pooled studies that assessed follow-up tests at same time points. Numbers of studies pooled in the subgroup meta-analyses at follow-up tests were small (three or four studies). Therefore, caution is needed when interpreting our results. Further RCTs assessing follow-up time points are required to confirm long-term effects of website and mobile application-based interventions.
Of seven studies that assessed treatment adherence as the proportion of participants of the intervention group who completed all sessions, four studies had 50% or greater completion rates, indicating that participants’ treatment completion rate in included studies was low. Some studies provided reminders to participants. However, various factors such as voluntary use, performance expectancy, effect expectancy, and facilitating conditions might influence user acceptance for technology [30]. Therefore, website and mobile application-based interventions should be developed considering factors that might influence user acceptance and treatment adherence other than reminders sent to participants.
As this review was based exclusively on studies in English, language bias should be considered. Moreover, since grey literature and unpublished studies were not included in this review, there might be a publication bias. As this review focused on website and mobile application-based interventions, results from interventions conducted combining face-to-face and online delivery were excluded.
CONCLUSION
This study updates integrated results on current evidence of website and mobile application-based interventions for adolescents and young adults with depression. We found that the most frequently used intervention strategy was ICBT and that most studies employed website-based interventions. Our meta-analysis showed a significant effect of overall website and mobile application-based interventions in reducing depressive symptoms at posttest. Subgroup meta-analyses showed significant effects of ICBT and website-based interventions. Studies that employed mobile application-based interventions were lacking. Therefore, more studies using mobile application are required. We recommend interventions using website for adolescents and young adults with depression. Our results suggest that ICBT might be effective. Because significant effects of website and mobile application-based interventions at long-term follow-ups were not confirmed, further RCTs are required to provide evidence on their long-term effects.